Osteoporosis is frequently identified only after a preventable fracture has already occurred. A recent BMJ review confirms this remains one of the most significant gaps in modern bone health care — and why earlier identification changes outcomes.
By Dr Taher Mahmud FRCP
Consultant Rheumatologist & Co-Founder, London Osteoporosis Clinic
Updated: May 2026
Key Takeaways
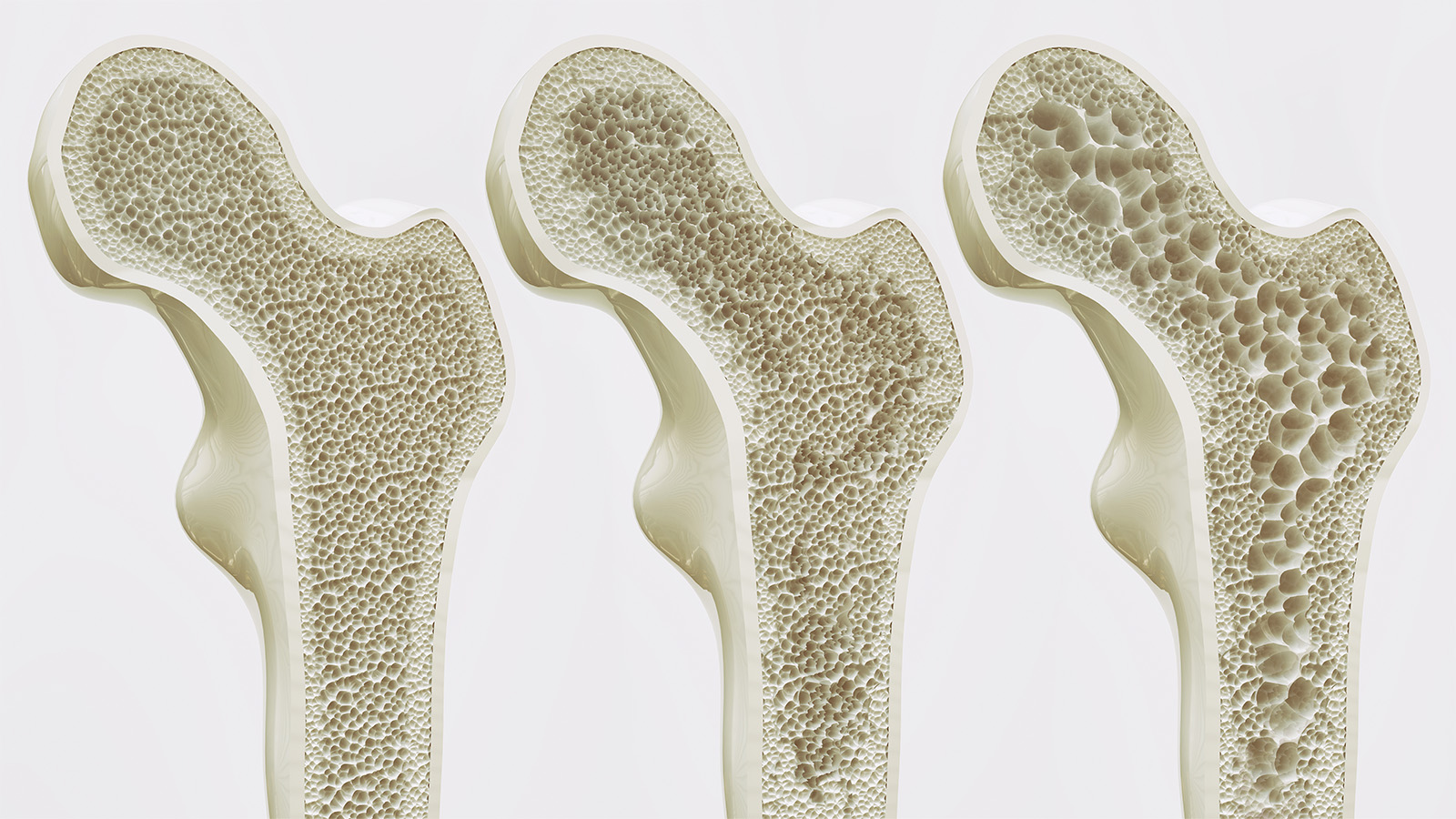
- Osteoporosis typically develops silently over many years — most people feel well while bone strength declines.
- A recent BMJ review [1] highlights that diagnosis is still too often made only after the first fracture.
- Fragility fractures carry serious consequences: reduced mobility, chronic pain, loss of independence, and increased mortality after hip fracture.
- Modern care increasingly focuses on earlier risk identification, DXA scanning, personalised fracture-risk assessment, and targeted intervention.
- Many fractures are preventable — the goal is to identify risk before bone strength has significantly declined.

Why Is Osteoporosis Still Being Found Too Late?
Bone loss develops quietly. People may feel entirely well for years while bone strength progressively declines — there are no reliable external signs until something breaks.
A recent review published in the BMJ [1] confirms what many clinicians working in bone health have recognised for years: osteoporosis remains underdiagnosed, undertreated, and too often identified only after a preventable fracture has already occurred.
The problem is structural. Osteoporosis does not produce symptoms in the way cardiovascular disease or diabetes might prompt investigation. Without a screening prompt — a risk factor, a concerned GP, a prior fracture — many patients are simply never assessed.
In the UK, there are more than 524,000 fragility fractures every year, with over 1,150 deaths per month linked to osteoporotic fracture [2]. Most of these fractures occur in people who had never been formally assessed.
What Are the Early Signs of Osteoporosis to Watch For?
Because osteoporosis is largely silent in its early stages, patients and clinicians need to look for indirect signals rather than waiting for obvious symptoms. These may include:
- Gradual loss of height (often unnoticed without measurement)
- Change in posture — increased thoracic kyphosis
- Reduced grip strength or confidence with physical activity
- Persistent back pain, particularly mid or lower thoracic
- A fracture after a fall from standing height or less
By the time these signs appear, bone strength has typically already declined significantly. This is precisely why proactive risk assessment matters — not because symptoms are present, but because their absence is no guarantee of normal bone health.
What Are the Consequences of a Fragility Fracture?
Fragility fractures — those occurring after minimal trauma, such as a fall from standing height — carry consequences that extend well beyond the fracture itself.
Hip fractures in particular are associated with significant mortality: up to 30% of patients die within one year [1]. Survivors frequently experience reduced mobility, loss of independence, and increased frailty. Vertebral fractures, though often less dramatic in presentation, can cause chronic back pain, height loss, and a substantially elevated risk of further fracture.
The encouraging reality is that the majority of fragility fractures are potentially preventable — provided bone health is assessed and addressed before bone strength has been critically compromised.
How Is Osteoporosis Assessment Changing in 2026?
Modern osteoporosis care is shifting towards earlier risk identification and personalised management. Key developments include:
- Earlier use of DXA scanning — the gold standard for measuring bone mineral density and generating T-scores and Z-scores
- FRAX and QFracture — validated tools for estimating 10-year fracture probability, integrating multiple clinical risk factors beyond bone density alone [3]
- Trabecular Bone Score (TBS) — an advanced analysis layered on top of standard DXA that assesses bone microarchitecture and quality
- Bone turnover markers — blood tests that help assess the rate of bone remodelling and monitor treatment response over time
- Structured exercise and nutritional optimisation — increasingly recognised as foundational rather than supplementary interventions
The shift in thinking is significant: it is no longer sufficient to diagnose osteoporosis after fracture and prescribe medication. The aim is to understand not only where bone density is today, but the direction of travel — and to intervene early enough that trajectory can be meaningfully changed.
How Has Osteoporosis Treatment Advanced?
Considerably. While bisphosphonates (such as alendronate and risedronate) remain widely prescribed, the treatment landscape now includes:
- Anabolic (bone-forming) therapies — such as teriparatide and romosozumab, which actively stimulate new bone formation rather than simply slowing its loss
- Sequential treatment strategies — where anabolic therapy is followed by anti-resorptive consolidation to preserve gains
- Denosumab — a targeted RANK-L inhibitor for those unable to tolerate bisphosphonates or requiring greater potency
- Personalised monitoring — structured reassessment and treatment review rather than indefinite prescribing
At the London Osteoporosis Clinic, the approach is reversal-first — focused on changing the bone health trajectory through nutrition, resistance training, metabolic optimisation, and targeted treatment where the clinical picture supports it — with the goal of actively improving bone strength, not merely slowing decline. The BoneRevive® programme typically achieves 8–12% bone mineral density improvement per year, measurable on serial DXA.
Who Should Not Wait Before Getting a Bone Health Assessment?
Earlier assessment is particularly relevant for individuals with recognised risk factors, even in the complete absence of symptoms. This includes:
- Women after menopause, particularly in the first 5–10 years
- Men over 50, especially with additional risk factors
- Individuals with a family history of osteoporosis or hip fracture
- Those on long-term corticosteroids or other bone-affecting medications
- People with inflammatory conditions such as rheumatoid arthritis or inflammatory bowel disease
- Individuals with low body weight, a history of amenorrhoea, or disordered eating
- Athletes with relative energy deficiency in sport (RED-S)
- Anyone noticing height loss, postural change, or unexplained back pain
If you recognise yourself in any of these categories, a structured bone health assessment is a sensible and proactive step — not a cause for alarm.
The LOC View
The window in which intervention is most effective is precisely the window in which the disease is silent. In clinical practice, we see patients at every stage — from those who have never had a fracture but carry significant latent risk, to those managing the aftermath of multiple vertebral fractures. The earlier we can assess bone trajectory and intervene appropriately, the more the pathway can offer. Waiting for a fracture is not a clinical strategy — it is a missed opportunity.
— Dr Taher Mahmud FRCP, Consultant Rheumatologist, London Osteoporosis Clinic
Frequently Asked Questions
At what age should I have a bone density scan?
NICE guidelines generally recommend DXA assessment for women over 65 and for younger individuals with risk factors. If you have recognised risk factors — family history, long-term steroid use, inflammatory conditions, or early menopause — earlier assessment is appropriate.
Can osteoporosis be reversed?
Bone loss associated with osteoporosis can be partially reversed with appropriate treatment. Anabolic therapies in particular can generate measurable new bone formation. Full return to peak bone mass is not typically achievable, but meaningful improvement in fracture risk is possible with a structured programme.
Is osteoporosis only a concern for older women?
No. While postmenopausal women carry the highest population-level risk, osteoporosis affects men, younger women with hormonal disruption, and individuals of any age with secondary causes such as long-term steroid use, malabsorption, or inflammatory disease.
What is the difference between osteoporosis and osteopenia?
Osteopenia describes bone mineral density below the normal range but not yet meeting the diagnostic threshold for osteoporosis (T-score between −1.0 and −2.5). It is not a disease in itself, but it warrants monitoring and, in some individuals, intervention — particularly when combined with other risk factors.
Taking the Next Step
Osteoporosis is common, but fragility fractures are not inevitable. Earlier identification, personalised assessment, and appropriate intervention — whether nutritional, pharmacological, or exercise-based — change outcomes in a meaningful and measurable way.
If you are concerned about your bone health, or if you fall into one of the higher-risk groups described above, the Bone Pathway™ at the London Osteoporosis Clinic offers a structured, consultant-led approach to assessment, diagnosis, and long-term management.
Book a bone health assessment →
References
- Hoong CWS, Saul D, Khosla S, Sfeir JG. Advances in the management of osteoporosis. BMJ. 2025;390. doi:10.1136/bmj-2024-081250
- Royal Osteoporosis Society. Key facts and figures about osteoporosis. Available at: theros.org.uk [Accessed May 2026]
- FRAX® Fracture Risk Assessment Tool. University of Sheffield. Available at: frax.shef.ac.uk/FRAX [Accessed May 2026]
This article is intended as general information only and does not replace individual medical assessment. If you have concerns about your bone health, please consult a qualified clinician.
Dr Taher Mahmud FRCP is a Consultant Rheumatologist and Co-Founder of the London Osteoporosis Clinic, based at The Shard, London SE1. He holds two US patents in osteoporosis reversal and prevention and is a Trustee of the Global Osteoporosis Foundation.
Medically reviewed by Dr Taher Mahmud FRCP | Last updated: May 2026