Polymyalgia rheumatica (PMR) causes severe muscle stiffness and pain, but what many patients don’t realise is that the condition itself — and especially the steroid medications used to treat it — accelerates bone loss. This guide explains why bone density screening is essential for anyone with PMR and what can be done to protect skeletal health.
- Polymyalgia rheumatica is an inflammatory condition that affects people over 50, causing severe muscle stiffness and pain around the shoulders and hips
- Corticosteroids — the mainstay treatment for PMR — accelerate bone loss and significantly increase fracture risk, especially in the first 3–6 months of therapy
- Bone density screening (DEXA scan) should be considered early in PMR treatment to establish a baseline and identify those at highest risk
- Combined strategies including adequate calcium and vitamin D, weight-bearing exercise, and optimised steroid dosing can substantially reduce bone loss in PMR patients
- Managing PMR well means protecting both muscle and bone — a comprehensive clinical review ensures neither is overlooked
Polymyalgia rheumatica is a serious inflammatory condition that impacts quality of life profoundly. Yet the damage it does to bone is often silent, unnoticed until a fracture occurs. At the London Osteoporosis Clinic, we work with many PMR patients to ensure that treatment focuses not only on controlling inflammation but also on preserving skeletal strength.

What Is Polymyalgia Rheumatica?
Polymyalgia rheumatica (PMR) is an inflammatory rheumatic condition that affects people aged 50 and over, with peak incidence in those over 70. It presents with sudden onset of severe aching, stiffness, and loss of strength, typically in the shoulders, neck, hip girdles, and thighs.
Classic presentations include:
- Severe morning stiffness lasting more than 45 minutes
- Inability to dress, comb hair, or rise from a chair
- Profound fatigue and malaise
- Unexplained weight loss
- Low-grade fever in some patients
The condition is autoimmune in origin — the body’s immune system inappropriately attacks the tissues surrounding joints and muscles. While the exact cause remains unknown, PMR is recognised as one of the most common systemic inflammatory diseases in older adults, with prevalence increasing sharply after age 60.
PMR can also occur alongside giant cell arteritis (temporal arteritis), a potentially sight-threatening vasculitis affecting blood vessels in the head and neck. This association makes rapid diagnosis and appropriate treatment critical.
Why Polymyalgia Rheumatica Damages Bone
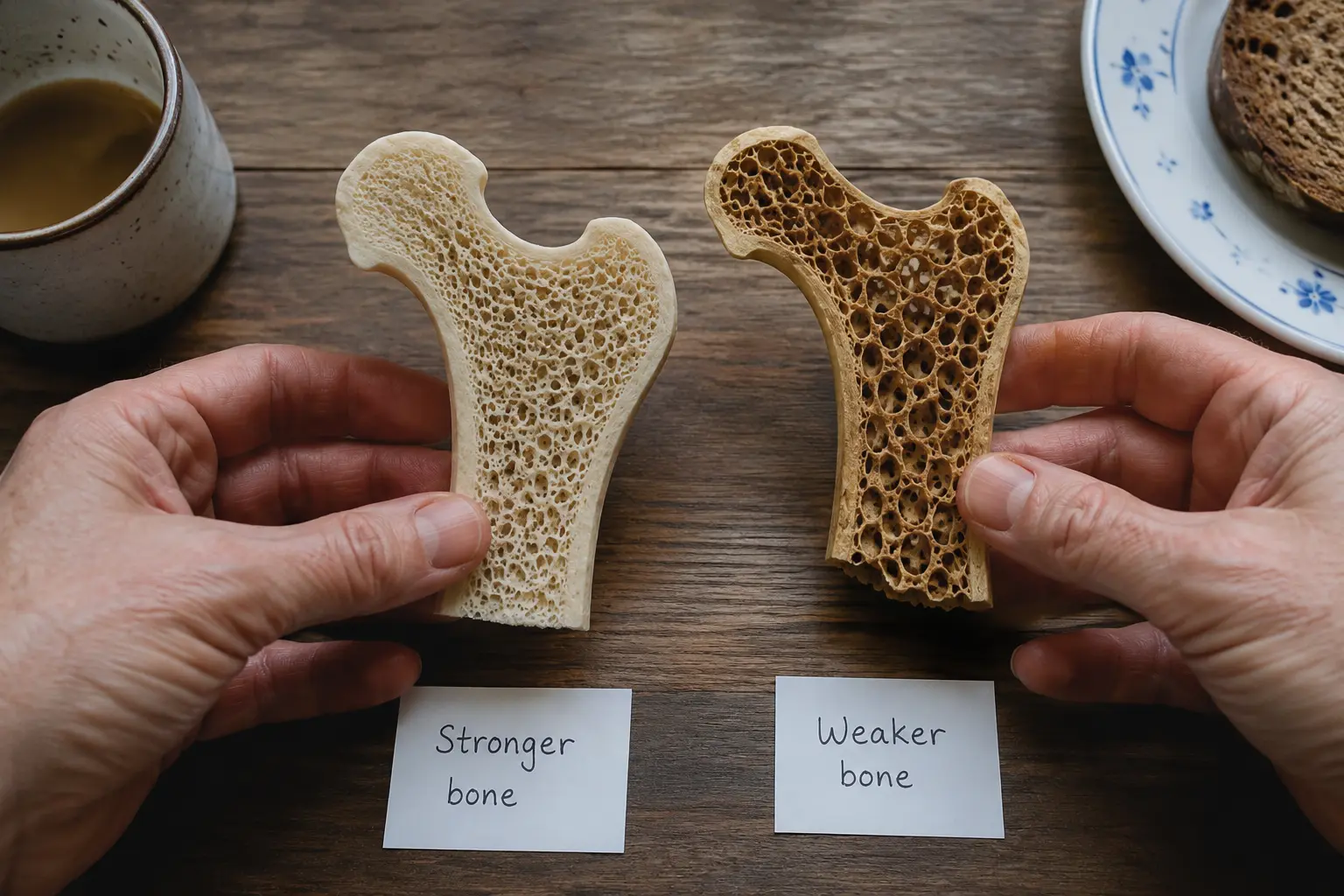
Bone loss in PMR occurs through multiple pathways. First, the inflammatory state itself drives bone resorption. Inflammatory cytokines — particularly TNF-alpha and IL-6 — activate osteoclasts (bone-resorbing cells) and suppress osteoblasts (bone-building cells). This creates a net loss of bone mineral density that can begin before treatment even starts.
Second, PMR severely limits physical activity. The pain and stiffness are so debilitating that many patients become sedentary, losing the weight-bearing activity essential for bone maintenance. Inactivity accelerates bone loss and contributes to muscle wasting — a particularly dangerous combination.
Third, and most significantly, the standard treatment for PMR — corticosteroid therapy — is inherently bone-toxic.
The Corticosteroid Problem: Why Bone Suffers
Corticosteroids, most commonly prednisolone, are the first-line and often only effective treatment for PMR. They rapidly suppress inflammation and restore quality of life — patients often report dramatic improvement within days. This efficacy is undeniable.
However, corticosteroids are profoundly damaging to bone:
- Direct osteoblast toxicity: Corticosteroids suppress the formation of new bone-building cells and accelerate their apoptosis (programmed cell death)
- Impaired calcium absorption: Steroids reduce intestinal calcium absorption and increase urinary calcium loss
- Secondary hyperparathyroidism: Chronic steroid use leads to compensatory overactivity of the parathyroid glands, further driving bone resorption
- Rapid initial loss: The most severe bone loss occurs in the first 3–6 months of steroid therapy — bone mineral density can decline by 5–10% in this window
- Dose-dependent effect: Higher steroid doses cause more rapid bone loss; cumulative lifetime steroid exposure matters
Studies show that PMR patients on corticosteroids have a two- to threefold increase in fracture risk compared to age-matched controls, even after adjustment for age and baseline bone density. Vertebral fractures — often asymptomatic — are particularly common.
Assessing Bone Density in Polymyalgia Rheumatica
Given the dual threat of inflammation and corticosteroid therapy, bone density assessment should be part of the clinical strategy for every PMR patient. The DEXA scan (dual-energy X-ray absorptiometry) is the gold standard.
Current guidelines recommend:
- Baseline DEXA scan at PMR diagnosis or when starting corticosteroids — to establish a starting point and identify patients already at risk
- Repeat DEXA scan at 1–2 years — to assess the rate of bone loss and guide further intervention
- Consideration of repeat scanning if steroid dose is reduced or changed significantly
Beyond bone density, clinical assessment should include evaluation of fracture risk factors: age, sex, prior fractures, family history of osteoporosis, and concurrent medications. Some patients benefit from fracture risk assessment tools (FRAX) to guide treatment decisions.
Protecting Bone While Treating Polymyalgia Rheumatica
Bone protection should begin at the same time as PMR treatment. A comprehensive strategy includes several pillars:
1. Optimise Steroid Dosing
Use the lowest effective dose of corticosteroid and taper as quickly as clinically safe. Most PMR patients can be managed on prednisolone 10–20 mg daily initially, tapering over 2–3 years. The goal is remission on the smallest maintenance dose possible.
2. Ensure Adequate Calcium and Vitamin D
PMR patients should aim for 1,000–1,200 mg of elemental calcium daily from diet and/or supplementation, and maintain vitamin D levels above 30 ng/mL. Deficiency is common and worsens steroid-induced bone loss.
3. Restore Physical Activity Cautiously
As PMR improves with treatment, weight-bearing and resistance exercise become critical. Walking, light resistance training, and balance work should be introduced gradually. Exercise not only preserves bone but also restores muscle strength and reduces fracture risk from falls.
4. Consider Bone-Protective Medications
Patients with baseline osteoporosis, rapid bone loss on DEXA follow-up, or prior fragility fractures may benefit from bisphosphonate therapy (alendronate, risedronate) or other bone-protective agents. These reduce fracture risk by 30–50% in corticosteroid-treated patients.
5. Address Modifiable Risk Factors
Smoking cessation, limiting alcohol, and ensuring adequate protein intake all support bone health. Some patients benefit from falls-prevention strategies to reduce fracture risk even if bone density is partially restored.
When to Seek Specialist Bone Health Assessment
All PMR patients deserve a clinical assessment that addresses bone health alongside inflammation control. This is particularly important for:
- Patients over 70 at PMR diagnosis
- Those requiring long-term corticosteroid therapy or high initial doses
- Patients with prior fragility fractures
- Those with additional risk factors (early menopause, low BMI, smoking history)
- Any patient in whom bone loss is accelerating on DEXA follow-up
The London Osteoporosis Clinic specialises in complex cases where inflammatory disease and bone health intersect. We work with your rheumatologist to ensure steroid therapy controls inflammation effectively while minimising skeletal damage.
Polymyalgia rheumatica is a condition where treatment is essential — corticosteroids transform lives by ending severe pain and restoring function. Yet this same treatment carries a skeletal cost that is often ignored until a fracture occurs. In clinical practice, managing PMR well means addressing both the inflammatory symptoms and the bones simultaneously. Every patient with PMR deserves a baseline bone density assessment and a clear strategy to protect skeletal health over the years of steroid therapy ahead. We regularly see PMR patients whose bone health has been silently compromised — and it is preventable. Book a consultation if you have PMR and want to ensure your bone health is optimised alongside your rheumatological care.
Does everyone with polymyalgia rheumatica develop osteoporosis?
Not everyone, but most PMR patients treated with long-term corticosteroids experience some degree of accelerated bone loss. The extent depends on baseline bone density, steroid dose and duration, age, and other risk factors. This is why baseline DEXA screening is so important — it identifies those at highest risk early, when intervention is most effective. Some patients maintain adequate bone density with careful management; others develop osteoporosis despite best efforts. Individual assessment is essential.
Can I prevent bone loss if I must take steroids for PMR?
Yes, substantially. While steroids cannot be avoided if PMR is to be treated, bone loss can be minimised through: (1) using the lowest effective steroid dose; (2) ensuring adequate calcium (1,000–1,200 mg/day) and vitamin D (target 30+ ng/mL); (3) maintaining weight-bearing and resistance exercise; (4) monitoring bone density with DEXA scans; and (5) considering bone-protective medications (bisphosphonates) for high-risk patients. These strategies together reduce fracture risk by 30–50%.
How long do I need to stay on steroids for polymyalgia rheumatica?
Most PMR patients require corticosteroid therapy for 2–3 years, though some need longer depending on disease activity. The goal is to use the lowest dose that controls symptoms, and to taper gradually as remission is achieved. Abrupt withdrawal can cause disease flare and adrenal insufficiency. Your rheumatologist will work with you to find the right balance between controlling PMR and minimising cumulative steroid exposure and side effects. During this time, bone health monitoring ensures you are not paying an unrecognised skeletal price for good disease control.
Should I take a bone-protective medication like alendronate if I have PMR?
Not necessarily everyone, but yes for many. Current guidelines recommend considering bisphosphonate therapy for PMR patients who: (1) have baseline osteoporosis on DEXA scan; (2) are over 65 and starting long-term corticosteroids; (3) show rapid bone loss on repeat DEXA scans; or (4) have prior fragility fractures. Your clinician can assess your individual fracture risk and advise whether a bone-protective medication is appropriate. The decision should be made early, ideally when PMR is diagnosed and steroid therapy begins.
Medically reviewed by Dr. Taher Mahmud, Consultant Rheumatologist and Co-Founder, London Osteoporosis Clinic. Dr. Mahmud has over 25 years of clinical experience in bone health and osteoporosis management.
This article is for informational purposes only and does not constitute medical advice. If you have polymyalgia rheumatica or concerns about your bone health, please consult with your rheumatologist or a bone health specialist. The London Osteoporosis Clinic can provide a comprehensive assessment of your skeletal health and work with your existing care team to optimise outcomes.
References:
[1] Gonzalez-Gay MA, et al. Polymyalgia rheumatica. Lancet. 2017. PubMed
[2] Soen S, et al. Prevention and treatment of glucocorticoid-induced osteoporosis. Journal of Bone and Mineral Metabolism. 2017. PubMed
[3] Buckley L, et al. American College of Rheumatology 2017 Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Arthritis & Rheumatology. 2017. PubMed
[4] Weyand CM, Goronzy JJ. Polymyalgia rheumatica and giant-cell arteritis. Annals of Internal Medicine. 2003. PubMed