Drug Treatment
At London Osteoporosis Clinic any drug is only used as part of holistic care.
Schematic illustration of the effect of an anabolic or a bone-building agent, followed by an antiresorptive on spine BMD (a) and on vertebral fracture incidence in postmenopausal women with high fracture risk, defined by previous vertebral fracture and low BMD (b).

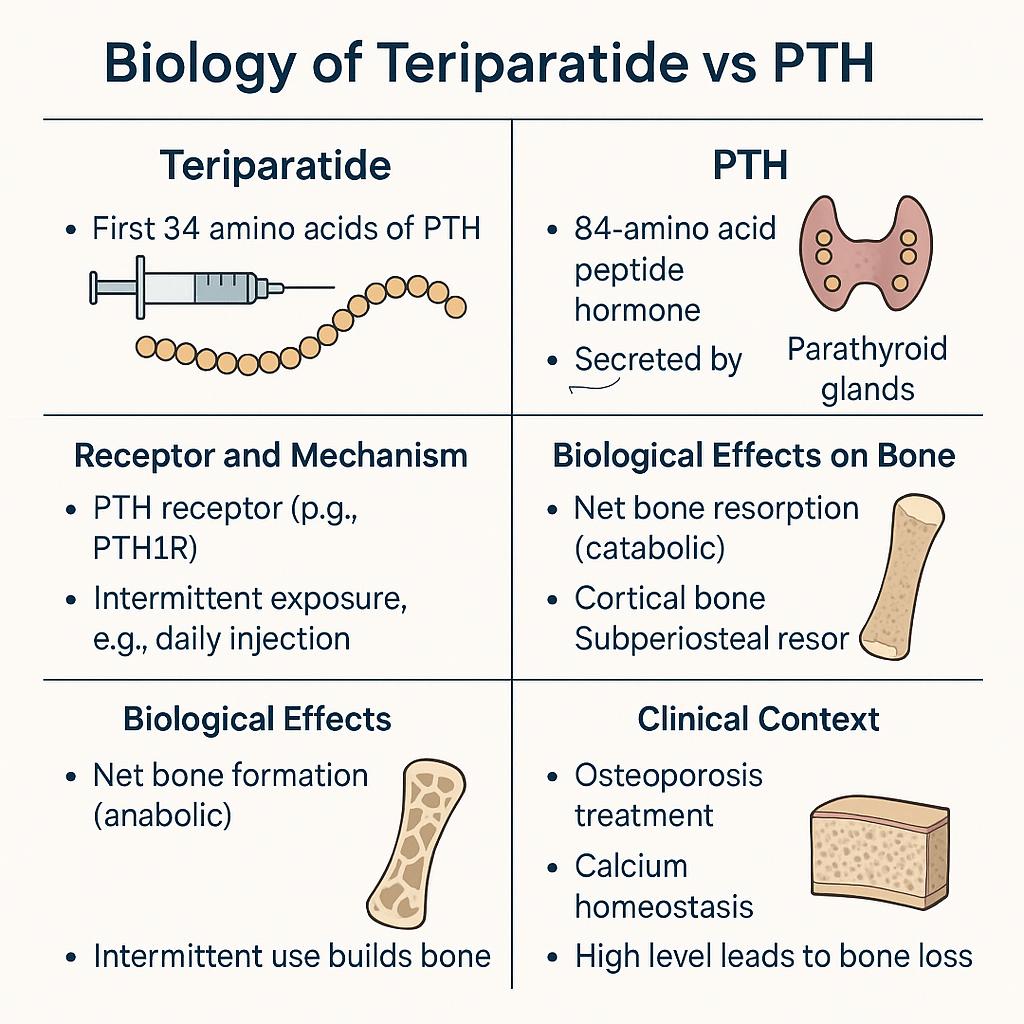
Understanding the Biology of Teriparatide vs PTH
At London Osteoporosis Clinic any drug is only used as part of holistic care.
This chart illustrates the biological differences between Teriparatide (a synthetic form of the first 34 amino acids of parathyroid hormone) and PTH, the body’s natural 84–amino acid hormone.
Teriparatide, given through daily injections, works by intermittently stimulating PTH receptors to promote new bone formation — making it an anabolic therapy ideal for osteoporosis treatment.
In contrast, continuous high levels of natural PTH lead to bone resorption (a catabolic effect), regulating calcium balance but potentially causing bone loss if sustained.
Our clinicians integrate these biological principles to optimize bone strength, reduce fracture risk, and maintain calcium homeostasis as part of a holistic, personalized care plan.
Bisphosphonates
There are several different kinds of bisphosphonate. Some are taken by mouth, while others are given by intravenous injection (a slow injection into a vein). Pamidronate, ibandronate and zoledronate are all types of bisphosphonates. Read more about bisphosphonates.
Teriparatide and parathyroid hormone
These help regulate calcium levels in your blood. They come in a ‘pen’ syringe and are injected under your skin. Read more about teriparatide and parathyroid hormone.
Denosumab
This is used for postmenopausal women who can not take bisphosphonates and in men who develop osteoporosis as a result of treatments for prostate cancer. Read more about denosumab.
Raloxifene
This is used to treat spinal osteoporosis in post-menopausal women following a fracture. It is given in a tablet form and taken daily. Read more about raloxifene.
Calcitonin
This is not used in the UK, only available as an injection to cut pain from pelvic and vertebral fractures in the time shortly after they occur. It should only be used for a most of 4 weeks. Read more about calcitonin.
Strontium ranelate
This is taken daily at least 2 hours before or after food. It comes as a powder which you mix with water.
HRT
It is mainly used as a short-term therapy for early post-menopausal women with increased fracture risk who have troublesome menopausal symptoms. Read more about HRT.
Calcium and vitamin D
Not getting enough calcium and vitamin D can increase your risk of fractures. You usually require supplements to help cut your risk and to promote better responses to other treatments for osteoporosis. Read more about calcium and vitamin D.
Zoledronate (zoledronic acid)
Zoledronate is a bisphosphonate used to treat osteoporosis. It helps strengthen bones and reduce the risk of fractures. It’s given as an intravenous infusion once a year.
You may be offered zoledronate if tablet treatments aren’t suitable, or after a hip fracture. Most people need calcium and vitamin D supplements during treatment.
Read more about zoledronate.
Romosozumab (Evenity®)
Romosozumab is a monthly injectable treatment for post-menopausal women with osteoporosis who are at high risk of fractures.
It works by increasing bone formation and reducing bone breakdown, helping to strengthen bones and lower the risk of new breaks.
Treatment lasts 12 months, followed by another osteoporosis medicine to maintain bone strength.
Read more about romosozumab.