At the European Congress of Rheumatology — EULAR 2026, held in London — Professor James Galloway of King’s College Hospital delivered a landmark session on early rheumatoid arthritis management. His conclusion was stark and evidence-backed: in RA, time is tissue. The biological window for disease modification begins closing at just 14 to 19 weeks from symptom onset — and every week of delay narrows the chance of drug-free sustained remission. For patients with joint pain, morning stiffness, or symmetrical swelling, early specialist review is not cautious medicine. It is urgent medicine.
- The biological window for disease modification in early RA closes at approximately 14–19 weeks from symptom onset — after which the probability of drug-free remission drops sharply.
- Remission is clinically and biologically distinct from low disease activity (LDA) — residual inflammation, even at low levels, continues to erode joints and accelerate bone loss.
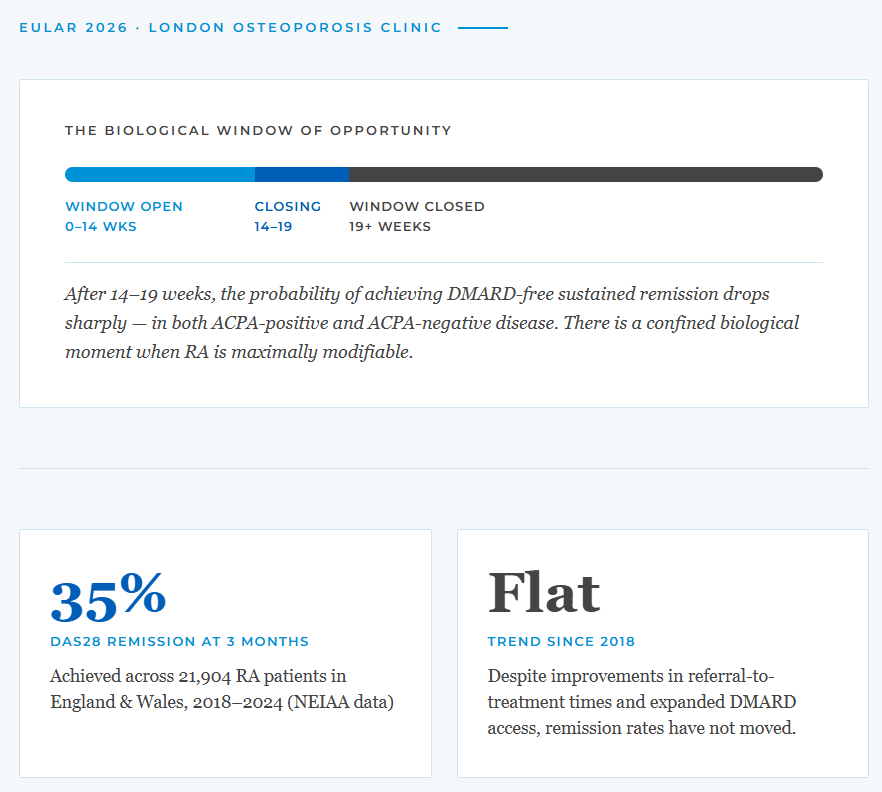
- NEIAA data from 21,904 patients shows only 35% of RA patients in England and Wales achieve remission at three months — a figure that has not improved since 2018.
- Glucocorticoids carry a significant bone cost: osteoporosis affects 42% of RA patients on steroids, versus 29% without — making early DMARD-driven remission the most bone-protective strategy available.

The Case for Remission: More Than Symptom Control
Professor Galloway opened by establishing what he called “The Therapeutic Ambition.” Remission in rheumatoid arthritis, he argued, is not simply the absence of symptoms. It is a fundamentally different biological state — one that prevents erosive joint damage, preserves long-term function, substantially lowers cardiovascular risk by dampening systemic inflammation, and critically, protects bone integrity.
The economic argument reinforced the clinical one. Patients in sustained remission show savings in direct medical costs of 19–52%, and in indirect productivity costs of 37–75%, compared with those in merely low disease activity. But there is a distinction that clinical practice has been slow to absorb:
“Remission is not the same as low disease activity. Even compared to LDA, remission delivers superior outcomes.” — Prof. James Galloway, EULAR 2026
This is not a semantic distinction. Low disease activity may feel like success in the clinic room — a patient with tolerable symptoms and a passable DAS28 score. But the data are unambiguous: residual inflammation, even at low levels, continues to erode joints, feed cardiovascular risk, and accelerate bone density loss. Remission must be the goal, not a secondary aspiration.
The Window of Opportunity: A Closing Door
The most important concept in the session was the “Window of Opportunity” — the early, confined period during which rheumatoid arthritis is most susceptible to disease modification. Drawing on data from the Leiden and ESPOIR cohorts of approximately 1,300 patients with early RA, Professor Galloway demonstrated that this window begins to close at just 14 to 19 weeks from symptom onset.
The Biological Window of Opportunity
0–14 wks
Closing
14–19
Window Closed
19+ weeks
After 14–19 weeks, the probability of achieving DMARD-free sustained remission drops sharply — in both ACPA-positive and ACPA-negative disease. There is a confined biological moment when RA is maximally modifiable.
This is a profound biological reality. The immune dysregulation that drives early RA is not a static process that worsens linearly. The disease passes through a phase of relative plasticity — a moment when the immune system has not yet committed to its destructive programme — before settling into a more entrenched state. Miss that window, and you are managing a fundamentally different disease.
Treat-to-Target: The Evidence Is Unambiguous
The landmark TICORA trial, published in The Lancet in 2004, remains the foundational proof of concept for treat-to-target strategy [1]. An intensive protocol — monthly DAS assessment, protocolised DMARD escalation, a target of DAS below 2.4 — achieved remission in 65% of patients at 18 months. The comparator, routine care, achieved 16%. X-ray progression fell by 67%, functional outcomes improved twofold, and the extra cost was zero.
These results were achieved with conventional synthetic DMARDs alone, before the biologics era. Since TICORA, the CAMERA, BeSt, and ARCTIC trials have all replicated and extended the finding across healthcare systems, populations, and treatment modalities. The conclusion is unsparing:
“Strategy matters as much as drug. If we have known this for twenty years — why hasn’t practice caught up?” — Prof. James Galloway, EULAR 2026
The Uncomfortable Truth: Remission Rates Have Not Improved
The National Early Inflammatory Arthritis Audit (NEIAA) provides the most complete picture of real-world RA care in England and Wales, capturing all new inflammatory arthritis referrals from 2018 to 2024. The audit tracks time from referral to first assessment, to DMARD initiation, and disease activity at three months. The verdict from 21,904 patients is sobering.
Achieved across 21,904 RA patients in England & Wales, 2018–2024 (NEIAA data)
Despite improvements in referral-to-treatment times and expanded DMARD access, remission rates have not moved.
Access to treatment has improved. Waiting times have shortened. But remission rates have remained stubbornly static at around one third. The implication is significant: the problem does not lie primarily within rheumatology services. It lies in what happens before patients reach those services.
The Pre-Rheumatology Bottleneck
NEIAA data analysed by Alveyn and colleagues (Rheumatology, 2025) confirms that symptom duration prior to referral is one of the strongest predictors of remission outcome. The probability of achieving remission at three months falls from approximately 37% when symptoms have been present for fewer than three months, to 30% when symptoms have persisted beyond a year. Post-COVID, this picture has deteriorated: pre-referral symptom duration has lengthened since the pandemic.
The predictors of not achieving remission identified in the NEIAA data are instructive:
- Longer symptom duration before referral to a rheumatologist
- Delayed DMARD initiation after first specialist assessment
- Higher baseline DAS28 score at presentation
- Younger age, female sex, and Black ethnicity — disparities that demand specific attention and equity-focused service design
As Professor Galloway put it: the bottleneck is pre-rheumatology. By the time patients reach a specialist, the window may already be closing — or closed.
Glucocorticoids — A Useful Bridge With a Real Bone Cost
The session also addressed the perennial question of glucocorticoid use in RA. Steroids remain attractive for their rapid symptom relief and their role as a bridge to DMARD effect. The GLORIA trial showed that 5mg/day of prednisolone improved DAS28 and slowed joint damage over two years in patients aged 65 and over. But at what cost?
The contemporary evidence on harm is sobering, and directly relevant to bone health monitoring in rheumatological practice:
- Osteoporosis: Affects 42% of RA patients on glucocorticoids versus 29% without — a 45% relative increase in fracture risk that requires proactive bone density monitoring and protective treatment
- Cardiovascular risk: Dose-dependent, with even 5mg/day or below associated with increased myocardial infarction and stroke risk
- Infection: GLORIA trial reported infection rates of 26% with GCs versus 16% without
- Overall harm composite: Any serious adverse event of special interest in GLORIA — 60% GC group versus 49% control, representing a 24% relative risk increase
The conclusion is not that glucocorticoids have no role. It is that achieving remission through effective DMARD strategy is simultaneously the most clinically powerful and the most bone-protective path forward. Sustained remission reduces GC dependence — and therefore protects bone density, cardiovascular health, and long-term function simultaneously.
For any patient with RA who is on or has been on corticosteroids, a DEXA bone density assessment is a standard part of clinical management that should not be deferred.
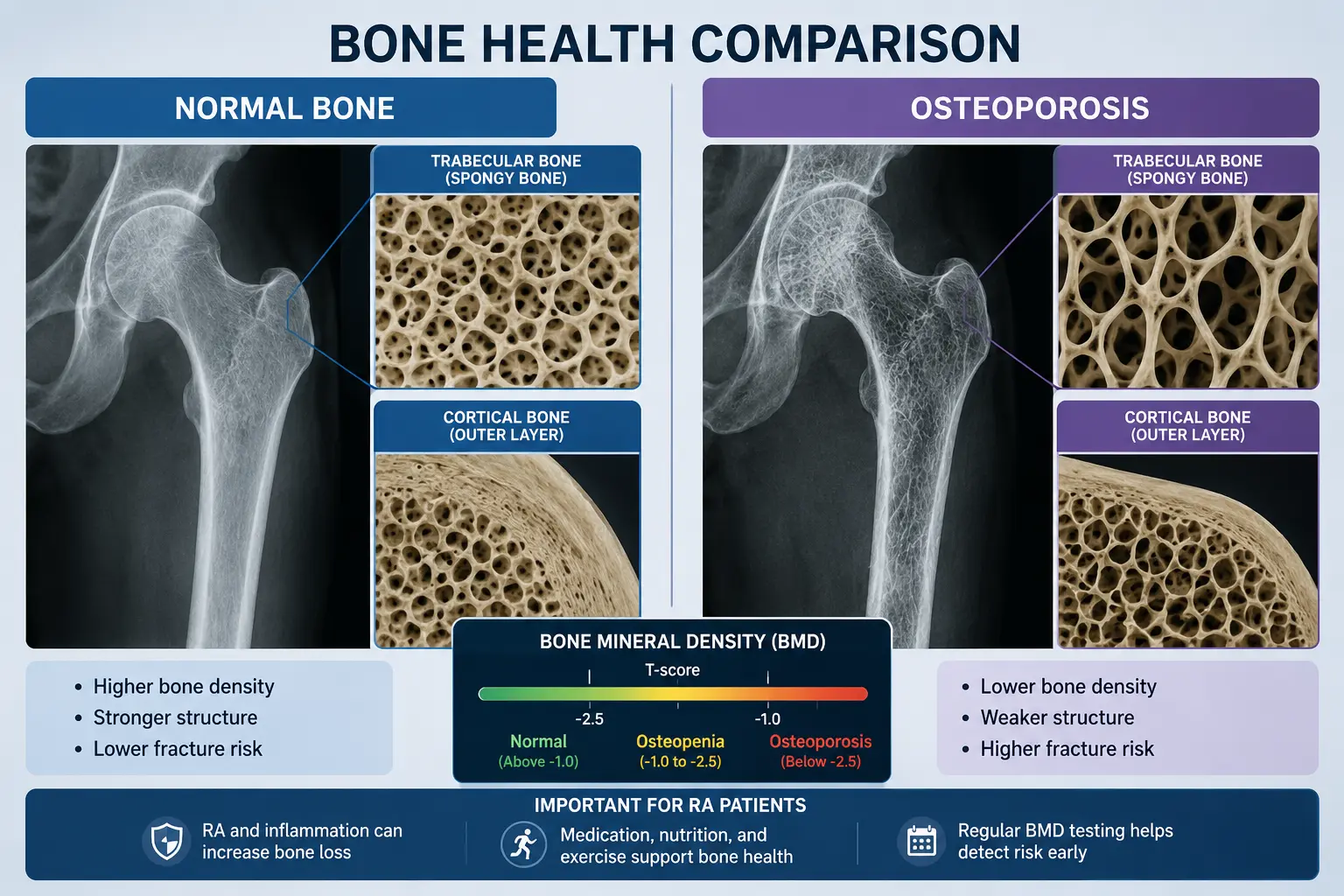
At London Osteoporosis Clinic, we see daily the skeletal consequences of undertreated inflammatory joint disease. Rheumatoid arthritis accelerates bone loss independently of steroid use, through direct osteoclast activation driven by the inflammatory cytokine environment. Patients who achieve and sustain remission recover measurably better bone density profiles than those who remain in persistent low disease activity.
The message from EULAR 2026 reinforces what we advocate clinically: the goal is not merely controlling symptoms but restoring biological normality. Treat early, treat to target, and monitor bone health as an integral dimension of rheumatological care — not an afterthought. Every referral delay costs something real.
What This Means If You Have Joint Symptoms
For GPs: a patient with morning stiffness lasting more than 30 minutes, symmetrical small joint swelling, and fatigue persisting beyond six weeks deserves urgent rheumatology review — not watchful waiting. The NICE two-week wait pathway for inflammatory arthritis exists and remains underused.
For patients: seek advice early. Do not accept that aching joints are an inevitable feature of ageing. Early RA is a treatable, potentially remissible disease when caught in the biological window. Waiting costs weeks that cannot be recovered.
Frequently Asked Questions
What is the “window of opportunity” in rheumatoid arthritis?
The window of opportunity refers to a confined early period — approximately the first 14 to 19 weeks from symptom onset — during which rheumatoid arthritis is most biologically susceptible to disease modification. Within this window, early DMARD treatment can achieve drug-free sustained remission in some patients. After the window closes, RA typically requires long-term medication management rather than potential cure.
What is the difference between remission and low disease activity in RA?
Remission means that inflammatory disease activity has been suppressed to a state where joint damage is not progressing and the body’s inflammatory burden is effectively normalised. Low disease activity (LDA) means symptoms are controlled but residual inflammation persists. Clinical trial data consistently show that remission produces superior outcomes — less radiographic progression, better function, lower cardiovascular risk, and better bone density preservation.
Does rheumatoid arthritis cause osteoporosis?
Yes — through two distinct mechanisms. First, the inflammatory cytokines that drive RA directly activate osteoclasts, the cells responsible for bone breakdown, independently of steroid use. Second, glucocorticoids used to manage RA cause substantial bone loss — osteoporosis affects approximately 42% of RA patients on corticosteroids, compared to 29% without. Bone density monitoring with a DEXA scan is recommended for all patients with established RA, particularly those on steroid treatment.
When should I see a rheumatologist about joint pain?
If you have symmetrical joint swelling or stiffness, morning stiffness lasting more than 30 minutes, fatigue, or joint pain persisting for more than six weeks, seek a GP review with a request for urgent rheumatology referral. The NICE two-week wait pathway applies to suspected inflammatory arthritis. Earlier referral translates directly into better remission outcomes.
Concerned about joint symptoms, bone health, or osteoporosis risk in the context of inflammatory disease? Our specialist team can assess both.
Medically Reviewed by Dr. Taher Mahmud
Dr. Taher Mahmud is a Consultant Rheumatologist and co-founder of the London Osteoporosis Clinic. He has over 20 years of clinical experience in inflammatory joint disease and bone health, and attended EULAR 2026 in London.
References
[1] Grigor C et al. (2004). Effect of a treatment strategy of tight control for rheumatoid arthritis (the TICORA study). The Lancet. Available at: PubMed.
[2] Alveyn E et al. (2025). Predictors of remission in early inflammatory arthritis: NEIAA analysis. Rheumatology. Available at: PubMed.
[3] Boers M et al. (2022). GLORIA trial — glucocorticoids in older patients with rheumatoid arthritis. Annals of the Rheumatic Diseases. Available at: PubMed.
This article summarises insights from the EULAR 2026 European Congress of Rheumatology and is intended for general information only. It does not constitute personalised medical advice. Always consult a qualified healthcare professional regarding your individual circumstances.