Gwyneth Paltrow has been open about her osteoporosis diagnosis and has shared elements of her approach to bone health through her Goop platform. Some of what she advocates is well-supported by clinical evidence. Some is not. A consultant rheumatologist reviews what she got right, what is missing, and what women with osteoporosis should actually prioritise.
- Gwyneth Paltrow disclosed an osteoporosis diagnosis linked to restrictive dieting and over-exercise — risk factors many women share but underestimate
- Some elements of her approach — vitamin D, dietary focus, weight-bearing exercise — align with clinical guidance; others lack robust evidence
- A DEXA scan is the only way to accurately diagnose and monitor osteoporosis; wellness protocols alone are not a substitute for clinical assessment
- For women concerned about bone density, the first step is not a supplement programme — it is a proper medical evaluation with a specialist
What Gwyneth Paltrow Has Said About Her Osteoporosis
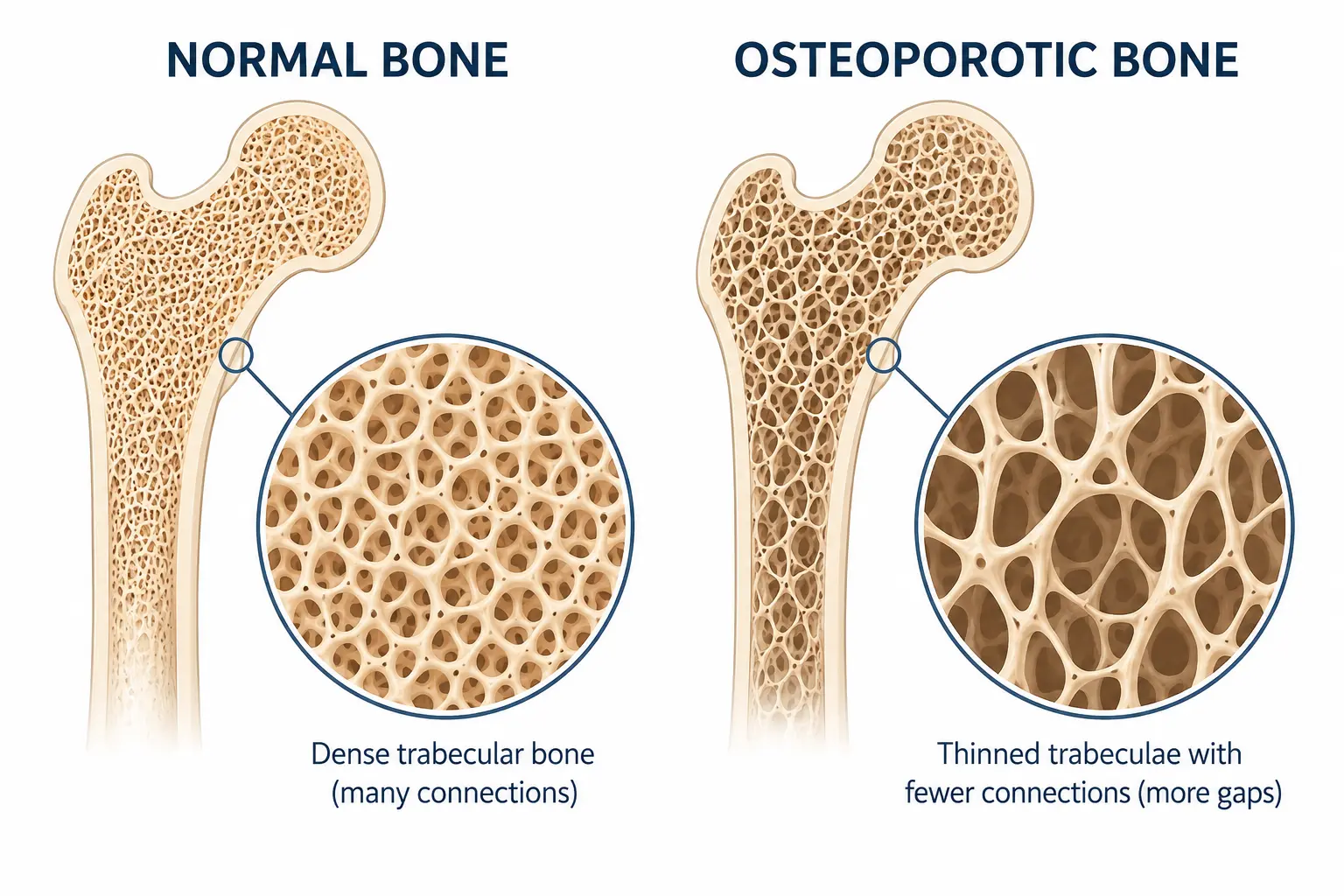
In 2023, Gwyneth Paltrow disclosed in interviews and through her Goop platform that she had been diagnosed with osteoporosis — a condition in which bone density falls to a level that significantly increases the risk of fracture. Her disclosure was notable because it challenged the common perception of osteoporosis as a condition that affects only elderly women. Paltrow was in her early fifties, visibly healthy, and physically active — yet her bone density had fallen below the diagnostic threshold.
She attributed her diagnosis in part to a period of extremely restrictive eating and over-exercise — specifically referencing a phase of her life characterised by low caloric intake and high-intensity training. This is clinically significant. Low energy availability — whether from disordered eating, over-training, or both — is one of the most powerful drivers of premature bone loss in women. The condition is formally recognised in sports medicine as part of the Female Athlete Triad, and it can affect women across all backgrounds, not only elite athletes.
Following her diagnosis, Paltrow spoke publicly about adjustments she had made: incorporating more protein, focusing on calcium-rich foods, taking vitamin D supplements, and undertaking weight-bearing exercise. She has also referenced various Goop wellness products in the context of bone health. Her story resonated widely — and for good reason. But celebrity health narratives require clinical scrutiny, and osteoporosis is a condition where the gap between wellness advice and medical reality can carry serious consequences.
We covered the full background of what Gwyneth Paltrow’s osteoporosis diagnosis means for patients in an earlier article. This piece focuses specifically on what she has done in response to it — and where the clinical picture diverges from the wellness narrative.
What She Got Right
Several elements of the approach Gwyneth Paltrow has described are clinically sound and consistent with mainstream medical guidance.
Vitamin D supplementation
Vitamin D is essential for calcium absorption, and deficiency is extremely common in the UK — particularly during autumn and winter. Public Health England recommends that all adults consider a daily supplement of 10 micrograms (400 IU) during these months, with higher doses appropriate for people with confirmed deficiency or established bone conditions. Advocating for vitamin D supplementation in the context of osteoporosis is well-supported by evidence [1].
Weight-bearing and resistance exercise
Exercise that loads the skeleton — walking, resistance training, certain forms of yoga — stimulates bone remodelling and helps maintain or modestly improve bone density. The Royal Osteoporosis Society recommends both impact exercise and progressive muscle-strengthening for people with osteoporosis, tailored to individual fracture risk [2]. Paltrow’s emphasis on exercise as part of bone health management is consistent with this guidance, provided it does not tip back into the over-training territory that contributed to her original diagnosis.
Dietary protein and calcium awareness
Adequate protein intake supports bone matrix formation, and calcium remains the primary structural mineral of bone. Increasing protein and calcium-rich food consumption after a period of dietary restriction is the correct direction of travel for someone recovering bone density from a low energy availability state. This is straightforward nutritional medicine, and it is right.
Where the Evidence Diverges
The wellness industry has a consistent pattern of presenting plausible adjacent truths alongside claims that are not supported by the same quality of evidence. In the context of osteoporosis, the most clinically significant gaps are these.
Collagen supplements
Collagen peptide supplements have been heavily promoted in the wellness space for bone and joint health. The evidence base is emerging but limited. Some small trials suggest modest benefits to bone density markers and joint pain, but the studies are typically short-term and not of sufficient quality to support replacing standard clinical interventions. Our detailed review of collagen versus calcium for bone strength examines the current evidence in full. The short answer: collagen supplements may offer some complementary benefit, but they are not a treatment for confirmed osteoporosis.
Restrictive dietary protocols
There is a significant tension within the Goop brand that is worth naming directly. Some of the dietary approaches promoted through Goop over the years — very low calorie phases, elimination protocols, extended fasting — are precisely the pattern that Paltrow herself identified as contributing to her bone loss. Low energy availability is not compatible with bone health. Any wellness approach that promotes sustained caloric restriction in women carries a real risk of compounding bone density loss, regardless of how it is branded.
Supplements without clinical oversight
Vitamin K2, magnesium, strontium and various botanical compounds are frequently referenced in wellness contexts for bone health. Some have supporting data; others do not. More importantly, supplementation in the context of confirmed osteoporosis should form part of a clinical management plan — not a self-directed protocol assembled from wellness content. Excess calcium supplementation without adequate vitamin D, for example, has been associated with cardiovascular risk in certain populations. Clinical supervision is not optional — it is protective.
What a Consultant Rheumatologist Would Actually Recommend
If a patient presents to the London Osteoporosis Clinic with a situation similar to Gwyneth Paltrow’s — a confirmed osteoporosis diagnosis in their early fifties, with a history of dietary restriction and over-exercise — here is what a clinical assessment would involve.
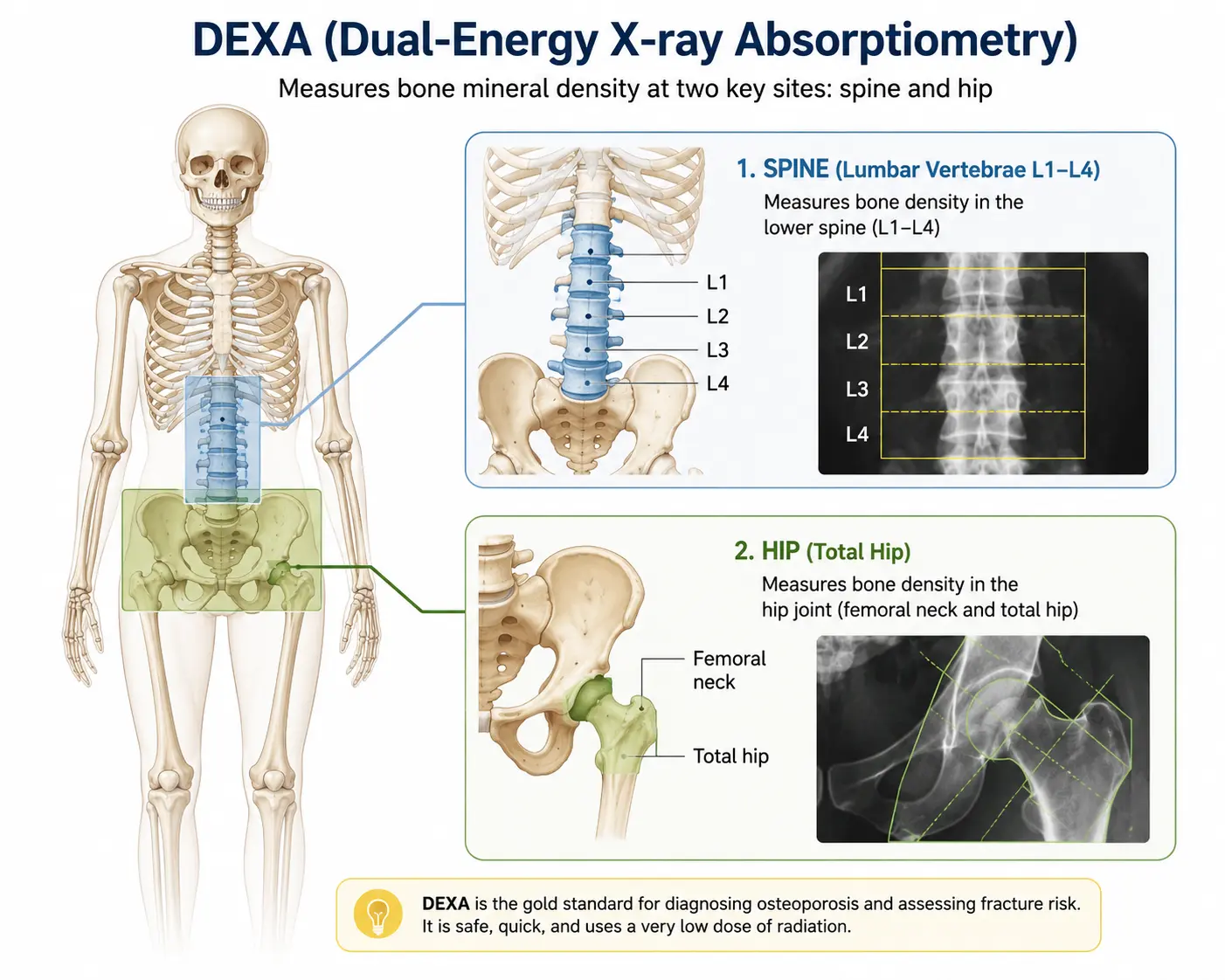
A DEXA scan to establish the current T-score at the spine and hip and to set a baseline for monitoring. Without this, you cannot know whether the condition is stable, improving or worsening in response to any intervention. We have written in detail about who should and should not have a DEXA scan, and what the results mean in practice.
Blood tests to assess calcium, vitamin D, parathyroid hormone and markers of bone turnover. In some cases, secondary causes of bone loss — thyroid disease, coeliac disease, renal disease — need to be excluded before a treatment plan is finalised.
A FRAX calculation — the internationally validated fracture risk assessment tool — to determine the ten-year probability of a major osteoporotic fracture and a hip fracture. This result directly informs the threshold for pharmaceutical intervention.
Pharmacological treatment where appropriate. For many patients with confirmed osteoporosis — particularly post-menopausal women with T-scores below -2.5 — lifestyle modification and supplementation alone are insufficient to adequately reduce fracture risk. First-line options include bisphosphonates (alendronate, risedronate), which have decades of evidence for reducing fracture risk. In higher-risk patients, anabolic therapies or denosumab may be appropriate. We cover all available osteoporosis treatments in our patient guides.
Ongoing monitoring. Osteoporosis is not addressed once and then set aside. Bone density should be rescanned periodically — typically every 2 years — to assess treatment response and guide decisions about continuing, changing or tapering therapy. The good news is that with the right treatment, osteoporosis can be reversed — but only when it is properly treated.
The Broader Lesson: Awareness Is Valuable, But Diagnosis Is Essential
Gwyneth Paltrow’s public disclosure about her osteoporosis has had a genuinely positive effect on awareness. Many women who read about her diagnosis will have considered their own bone health for the first time — and some of those women will have sought medical advice as a result. That is a real public health benefit and should be acknowledged.
The risk, however, is that a celebrity-driven wellness narrative creates the impression that osteoporosis can be managed through lifestyle and supplement choices alone, without requiring clinical investigation. For women at elevated risk — post-menopausal, with a history of dietary restriction, steroid use, family history of fracture, or previous low-trauma fracture — the most important step is not a supplement stack. It is an accurate diagnosis followed by a treatment plan that is calibrated to their actual fracture risk.
Gwyneth Paltrow has a bone specialist, whether or not she discusses that in public. You should too.
Gwyneth Paltrow did something genuinely useful by making her diagnosis public — she put osteoporosis in front of an audience that often does not think of it as relevant to them. But we see patients regularly who have been following wellness protocols for months or years and have no idea what their actual bone density is. A DEXA scan takes fifteen minutes. It tells you what no supplement label can. My concern with the wellness approach to osteoporosis is not that it is entirely wrong — some of it is directionally correct — it is that it can delay the clinical assessment that determines whether pharmaceutical intervention is needed. For a woman in her early fifties with a T-score below -2.5, lifestyle changes and supplements alone are very unlikely to be sufficient to prevent fracture. That conversation needs to happen in a clinic.
Concerned about your bone health? Get a proper clinical assessment.
A DEXA scan and specialist consultation at the London Osteoporosis Clinic gives you a complete picture — and a real clinical plan, not a wellness protocol.
Frequently Asked Questions
What caused Gwyneth Paltrow’s osteoporosis?
Gwyneth Paltrow has attributed her osteoporosis diagnosis in part to a period of restrictive dieting and over-exercise earlier in her life — a pattern that leads to what clinicians call low energy availability. When the body is consistently undernourished relative to energy expenditure, it down-regulates bone-building activity as part of a broader metabolic adaptation. This is a well-recognised cause of premature bone loss in women and is formally described as part of the Female Athlete Triad in sports medicine. It is not limited to elite athletes; it can affect any woman who has sustained very low caloric intake over a significant period of time.
Are the supplements promoted by Gwyneth Paltrow for bone health evidence-based?
Some have supporting evidence; others do not. Vitamin D supplementation is well-supported and widely recommended in NHS and clinical guidelines. Calcium through dietary sources is also evidence-based, though calcium supplements in high doses without adequate vitamin D carry some caveats. Collagen peptide supplements have emerging but limited data and are not supported by the same quality of evidence as established pharmaceutical treatments. For confirmed osteoporosis, supplementation alone — regardless of brand or formulation — is not sufficient to adequately reduce fracture risk. A clinical assessment is the essential first step to determine whether pharmaceutical treatment is warranted.
I have been following a wellness approach to bone health. Do I still need to see a doctor?
If you are post-menopausal, have a history of dietary restriction, have taken long-term steroids, have a family history of osteoporosis, or have experienced any low-trauma fracture, you should have a clinical assessment regardless of your current supplement or lifestyle protocol. A DEXA scan is the only way to accurately diagnose osteoporosis and establish a baseline for monitoring. Lifestyle and dietary approaches have a genuine role in bone health, but they cannot replace knowing your actual bone density. A consultation at the London Osteoporosis Clinic can confirm your risk level and whether any treatment is appropriate.
Medically reviewed by Dr. Taher Mahmud, Consultant Rheumatologist and Co-Founder, London Osteoporosis Clinic. Dr. Mahmud has over 25 years of clinical experience in bone health and osteoporosis management.
This article is for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare professional regarding any health concerns or before making changes to your treatment plan.