Sally Field was diagnosed with osteoporosis in her mid-fifties and went on to become the most recognised face of bone health advocacy in the world — the long-running spokesperson for Boniva, a once-monthly bisphosphonate. Her campaign helped millions of women take osteoporosis seriously for the first time. A consultant rheumatologist examines what her story tells us, how Boniva actually works, and what women diagnosed today need to know about their treatment options.
- Sally Field was diagnosed with osteoporosis and became the spokesperson for Boniva (ibandronate) — a once-monthly oral bisphosphonate — bringing bone health to a mainstream audience
- Bisphosphonates remain the evidence-based first-line treatment for osteoporosis and have decades of data supporting their ability to reduce fracture risk
- Monthly ibandronate and weekly alendronate work differently — comparative evidence favours alendronate for hip fracture reduction, and treatment choice should always be individualised
- Celebrity advocacy raises awareness, but diagnosis and treatment decisions require a DEXA scan and a specialist consultation — not a TV advertisement
How Sally Field Brought Osteoporosis Into the Mainstream
When Sally Field began appearing in Boniva advertisements in 2006, osteoporosis was still widely perceived as an inevitable, untreatable consequence of ageing — something that happened to elderly women, not to active, healthy women in their fifties. Field changed that perception almost single-handedly. By speaking openly about her own diagnosis, she made the condition visible, relatable and — crucially — treatable in the public imagination.
The impact was real. Osteoporosis screening rates rose during the years of the Boniva campaign, and the number of women discussing bone health with their GPs increased measurably. In a condition where the majority of fractures occur in people who have never been tested or treated, awareness campaigns that reduce the gap between diagnosis and intervention save lives and prevent disability.
Field has continued to speak about bone health over the years, and her advocacy has never been limited to product promotion. She has consistently emphasised that osteoporosis is a medical condition requiring proper clinical management — not just a lifestyle issue to be addressed with supplements and exercise. That message is clinically correct, and it matters.
For readers who are newer to the topic, our overview of celebrities with osteoporosis puts Sally Field’s story in a broader context of public figures who have helped shift awareness of this underdiagnosed condition.
What is Boniva and How Does it Work?
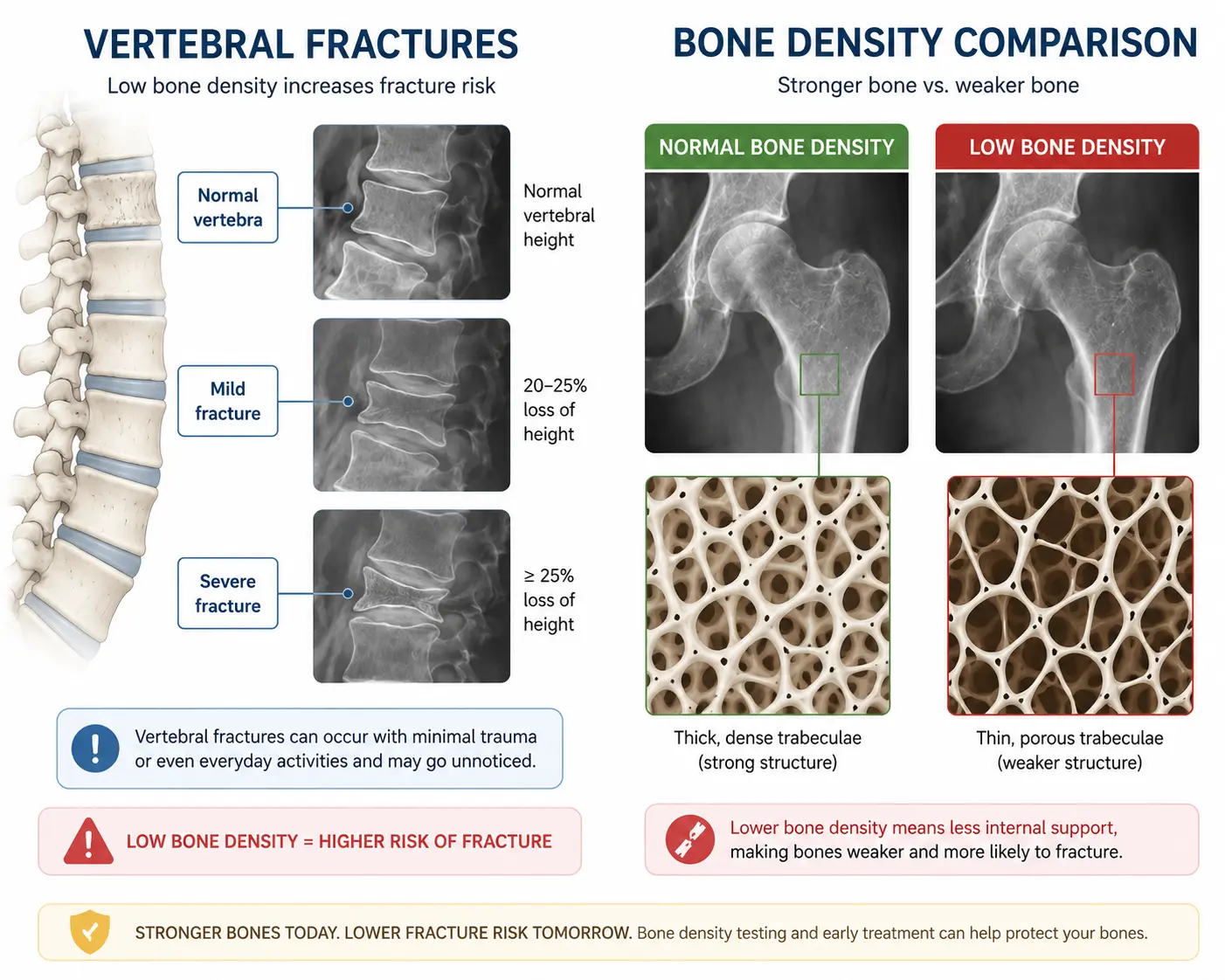
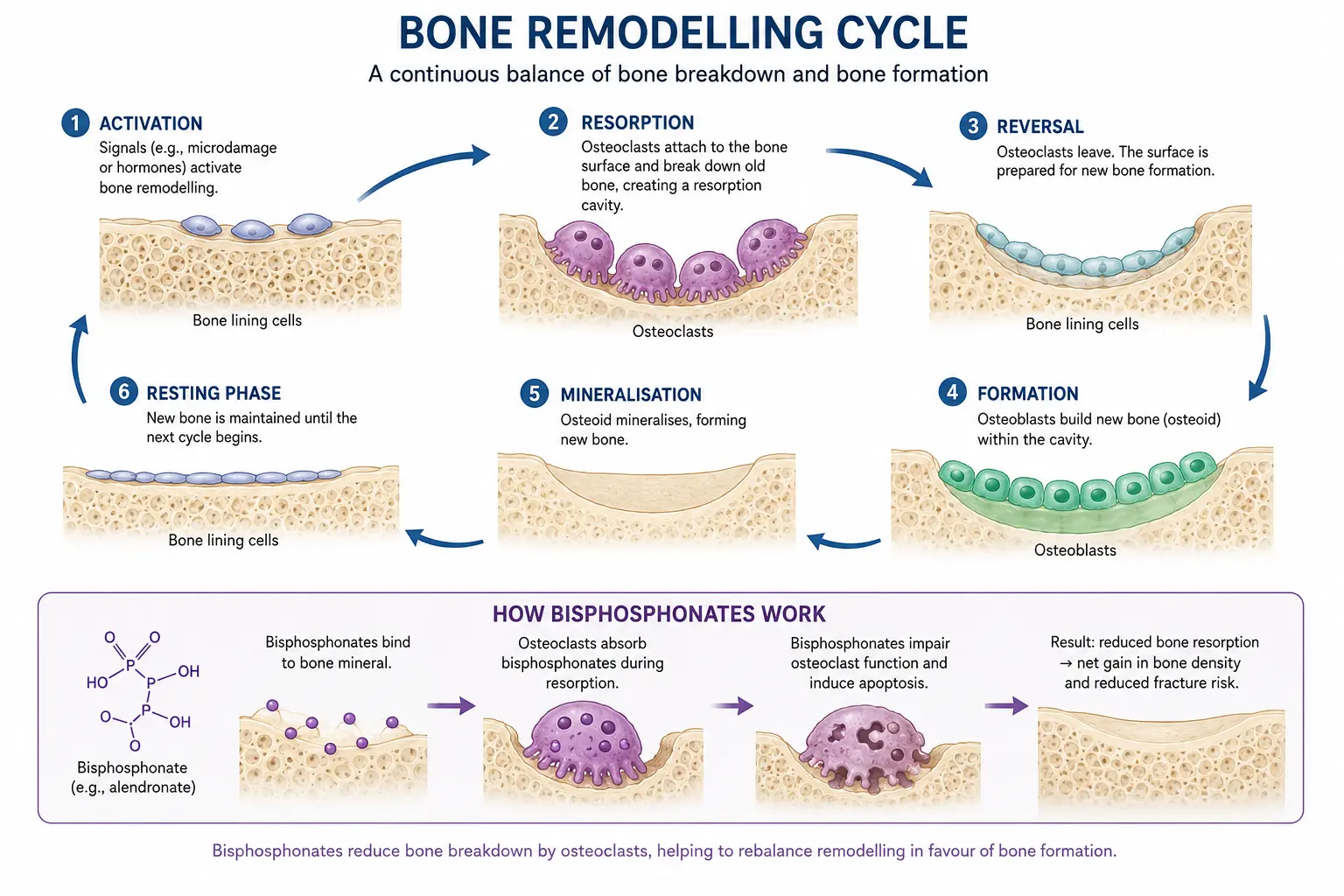
Boniva is the brand name for ibandronate, a bisphosphonate medication approved for the treatment and prevention of postmenopausal osteoporosis. Bisphosphonates are the most widely prescribed class of drugs for osteoporosis globally, and they work by inhibiting osteoclast activity — the cells responsible for breaking down old bone tissue in the normal cycle of bone remodelling.
In healthy bone, osteoclasts and osteoblasts (bone-building cells) work in balance. In osteoporosis, the resorption side of this equation is overactive relative to formation — bone is broken down faster than it is rebuilt. Bisphosphonates bind to bone mineral surfaces and reduce osteoclast activity, slowing the rate of bone loss and, in many patients, achieving modest improvements in bone density over time.
What distinguished Boniva from earlier bisphosphonates was its dosing schedule. Where alendronate (the most widely used bisphosphonate in the UK, sold as Fosamax) requires weekly oral dosing, ibandronate is taken once monthly. For many patients, monthly dosing improved adherence — missing a weekly pill is easy; remembering a monthly pill felt more manageable. This was the primary patient-facing benefit of Boniva, and it was a genuine clinical consideration. Poor adherence to bisphosphonate therapy is one of the most significant drivers of treatment failure in osteoporosis, so anything that improves the likelihood of patients taking their medication consistently has real clinical value [1].
Boniva vs Other Bisphosphonates: What the Evidence Shows
This is where the clinical picture becomes more nuanced — and where the advertising narrative and the medical evidence begin to diverge slightly.
All bisphosphonates reduce fracture risk, but the evidence base is not identical across agents. Alendronate (weekly) and risedronate have the largest and most robust evidence base, with randomised controlled trial data demonstrating significant reductions in vertebral fracture risk (40–50%), non-vertebral fracture risk (20–30%), and — critically — hip fracture risk. The hip fracture data is particularly important because hip fractures carry the highest morbidity and mortality of any osteoporotic fracture.
Ibandronate (Boniva) has strong evidence for vertebral fracture reduction, but its evidence for hip fracture reduction is less robust than that of alendronate or risedronate. This is not a reason to dismiss it — for patients with primarily vertebral disease, or for those who cannot tolerate weekly dosing, ibandronate remains a clinically appropriate option. But it does mean that treatment choice should be driven by individual clinical circumstances, not by advertising exposure [2].
In the UK, the National Osteoporosis Guideline Group (NOGG) and NICE position alendronate as the first-line oral bisphosphonate for most patients, primarily because of its comprehensive fracture reduction data and cost-effectiveness. Ibandronate is a valid alternative — particularly for patients who experience gastrointestinal side effects with alendronate, or who strongly prefer monthly dosing.
Intravenous bisphosphonate: zoledronic acid
For patients who cannot tolerate any oral bisphosphonate — due to oesophageal conditions, swallowing difficulties, or persistent gastrointestinal symptoms — intravenous zoledronic acid (Aclasta) is an excellent alternative. It is administered once yearly via infusion and has strong fracture reduction data across all skeletal sites including the hip. It is also the preferred option for patients with poor adherence to oral medication. We discuss the full range of osteoporosis treatments in detail in our patient guides.
What Sally Field’s Advocacy Got Right
Setting aside the commercial context, several things about Sally Field’s approach to her osteoporosis diagnosis deserve genuine credit.
She sought treatment. This sounds obvious, but in a condition where the majority of people who sustain a first fragility fracture never receive a bone density assessment or treatment in the subsequent year — the so-called treatment gap — deciding to engage with the medical system and take medication is a significant step. Millions of women who saw her advertisements and asked their doctors about bone health for the first time owe something to that decision.
She engaged consistently over time. Osteoporosis is a chronic condition requiring ongoing management, not a one-off intervention. Field’s sustained involvement in awareness campaigns — spanning nearly two decades — reflects the reality that bone health management is a long-term commitment, not a short-term fix.
She spoke about prevention, not just treatment. Her messaging consistently included the importance of calcium, vitamin D, weight-bearing exercise and regular monitoring — all of which align with evidence-based clinical guidance. The combination of pharmaceutical treatment and lifestyle modification is exactly what clinical guidelines recommend, and she communicated it accessibly to a non-medical audience.
The Limits of Celebrity-Led Health Campaigns
The same caveat that applies to Gwyneth Paltrow’s wellness narrative — and to any celebrity health story — applies here too, albeit in a different form. Where wellness influencers risk overclaiming for unproven supplements, pharmaceutical advertising risks creating the impression that one specific drug is the default answer for every patient.
Osteoporosis treatment is not one-size-fits-all. A 55-year-old woman with a T-score of -2.6, no prior fractures and no significant comorbidities has a different treatment landscape than a 72-year-old with a previous hip fracture and renal impairment. The right bisphosphonate, the right dosing route, the right duration of therapy and whether pharmaceutical treatment is indicated at all — these are clinical decisions that require a full assessment, not a prescription shaped by television exposure.
Understanding that osteoporosis can be reversed with proper treatment is the right starting point. But the treatment plan itself must be personalised.
What a Full Bone Health Assessment Involves at the London Osteoporosis Clinic
For a patient presenting with a new osteoporosis diagnosis — or for a woman in her fifties who has never been assessed but recognises the risk factors — a comprehensive evaluation at the London Osteoporosis Clinic includes the following.
DEXA scanning of the lumbar spine and hip, providing T-scores that define bone density relative to a young adult reference population. This is the diagnostic standard and the only reliable way to confirm osteoporosis, distinguish it from osteopenia, and set a baseline for monitoring treatment response. Our guide to who should have a DEXA scan covers the indications in full.
FRAX assessment — the validated fracture risk tool — which incorporates age, BMI, prior fracture history, parental hip fracture, steroid use, secondary osteoporosis causes, alcohol consumption and smoking status to generate a ten-year fracture probability. This figure, combined with the DEXA result, determines whether treatment is recommended.
Bloods to exclude secondary causes of osteoporosis and to confirm adequate vitamin D levels before starting any bisphosphonate therapy. Treating osteoporosis with bisphosphonates in the context of uncorrected vitamin D deficiency is a common and avoidable error.
Treatment discussion covering all appropriate options — oral bisphosphonates, intravenous bisphosphonates, denosumab, anabolic therapies — with the evidence, benefits, risks and practical considerations for each discussed transparently with the patient.
Monitoring plan with repeat DEXA imaging at agreed intervals to assess treatment response and inform decisions about continuation or change of therapy.
Sally Field did more for osteoporosis awareness than most public health campaigns have managed in decades. The Boniva advertisements reached an audience that clinical guidelines never could. But when patients come to us having seen those advertisements — or having read about Gwyneth Paltrow, or having found us through a Google search — the first thing we do is not write a prescription. We assess. We look at fracture risk individually. We consider which treatment is actually the right choice for that specific patient. Bisphosphonates are excellent drugs when used correctly. Alendronate remains our first-line oral option for most patients because the hip fracture data is stronger. Some patients do better on monthly ibandronate or annual zoledronic acid, depending on their circumstances. The point is that the decision is made in a consultation, not by a television advertisement — however well-intentioned it may be.
Ready to understand your bone health properly?
A DEXA scan and specialist consultation at the London Osteoporosis Clinic gives you an accurate diagnosis, a personalised fracture risk assessment and a treatment plan built around you — not a one-size-fits-all approach.
Frequently Asked Questions
Is Boniva (ibandronate) still used for osteoporosis in the UK?
Yes, ibandronate is still available and used in the UK for postmenopausal osteoporosis, though it is not the first-line choice in NICE or NOGG guidelines. Alendronate (weekly oral) is the preferred first-line bisphosphonate for most patients in the UK because of its broader fracture reduction evidence — including hip fracture — and its cost-effectiveness. Ibandronate is an appropriate alternative for patients who cannot tolerate alendronate due to gastrointestinal side effects, or for those who strongly prefer monthly dosing. The right choice depends on your individual clinical profile and should be discussed with a specialist.
What is the difference between Boniva and alendronate for osteoporosis?
Both are bisphosphonates that reduce bone resorption and lower fracture risk, but they differ in dosing schedule and evidence base. Alendronate is taken weekly and has strong evidence for reducing vertebral, non-vertebral and hip fractures. Ibandronate (Boniva) is taken monthly and has robust evidence for vertebral fracture reduction, but its hip fracture evidence is less comprehensive. For most patients in the UK, alendronate is the first recommendation. Ibandronate is a valuable alternative for patients who prefer monthly dosing or who cannot tolerate weekly alendronate. A specialist can assess which is more appropriate for your circumstances.
How do I know if I need treatment for osteoporosis — or just monitoring?
The decision is based on two things: your bone density (measured by DEXA scan) and your ten-year fracture risk (calculated using the FRAX tool). Osteoporosis is confirmed when the T-score falls below -2.5. However, treatment is not automatic at that threshold — it depends on your age, fracture history, and other risk factors. Some patients with T-scores in the osteopenia range (between -1.0 and -2.5) may also benefit from treatment if their fracture risk is elevated. Equally, some patients with confirmed osteoporosis and low fracture risk may be managed with lifestyle measures and close monitoring rather than immediate pharmaceutical treatment. This assessment needs to be done properly with a specialist — a DEXA result alone is not the whole picture.
Medically reviewed by Dr. Taher Mahmud, Consultant Rheumatologist and Co-Founder, London Osteoporosis Clinic. Dr. Mahmud has over 25 years of clinical experience in bone health and osteoporosis management.
This article is for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare professional regarding any health concerns or before making changes to your treatment plan.